PROCEDURAL SEDATION USMLE and MEDSCAPE
I.
Indications. Anxiolysis, sedation, amnesia, and
analgesia during potentially anxiety provoking or painful procedures (eg,
fracture and dislocation reduction, I&D, burn or wound debridement, LP,
pediatric laceration repair, or pediatric diagnostic study).
II. Contraindications.
Lack of experienced personnel, serious co-morbid pulmonary or
cardiac disease (ASA class III-V), lack of proper airway and monitoring
equipment, known medication allergy, a meal within 4 hours and liquids within 2
hours (recent data suggests that fasting does not alter the risk of
aspiration), and patient intoxication.
III. Equipment. Cart
with resuscitation drugs and age-appropriate airway equipment, cardiac monitor,
O2 source, nasal cannula (used routinely) and BVM (if
hypoventilation), pulse oximeter (and capnography if available), IV access,
suction equipment, and reversal agents (naloxone and flumazenil).
IV. Procedure
A.
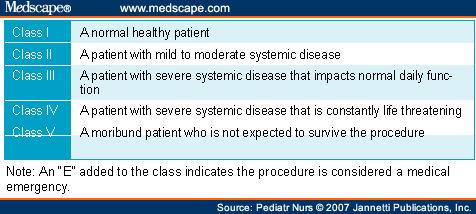
Perform a thorough
history and physical examination and patient assessment. Assign patients to a
physical status classification (Table 4–1). Sedation and analgesia in the ED
normally should be limited to patients in classes I and II.
B.
Explain the procedure
to the patient or guardian and gain informed consent.
C.
Connect patient to
appropriate monitoring equipment and assemble experienced personnel.
D.
Select analgesic,
sedative-hypnotic, or dissociative anesthetic, depending on the indication
(Table 4–2). Examples include adult procedure (etomidate or fentanyl and midazolam); pediatric procedure (ketamine with
atropine 0.01 mg/kg to maximum 0.3 mg +/- glycopyrrolate 0.005mg/kg to maximum
0.25 mg for secretions); and pediatric diagnostic procedure (ketamine or
midazolam).
E.
Have airway equipment
and reversal agent (naloxone for opiates and flumazenil for benzodiazepines) at
the bedside.

 |
V.
Complications
A.
Respiratory depression and hypoxia. Prevent with proper dosing,
application of O2, and if needed, positive pressure ventilation
(PPV).
B.
Laryngospasm. Give succinylcholine to
relieve spasm and then PPV.
C.
Rigid chest syndrome is a complication of administration of high
doses of fentanyl, which causes difficulty breathing due to chest wall muscle
spasm. Use IV naloxone to attempt reversal of fentanyl. If no improvement, use
succinylcholine and PPV.
D.
Vomiting with aspiration. Have suctioning set up and turn the
patient on their side if vomiting occurs.
E.
Prolonged sedation. Prevent with proper dosing and avoidance of
mixing multiple agents.

sources: USMLE and Medscape
December 30, 2016
